A FINDRISC-based diabetes risk assessment prototype that replaces a static score with a real-time what-if simulator and a ranked, patient-specific intervention plan.
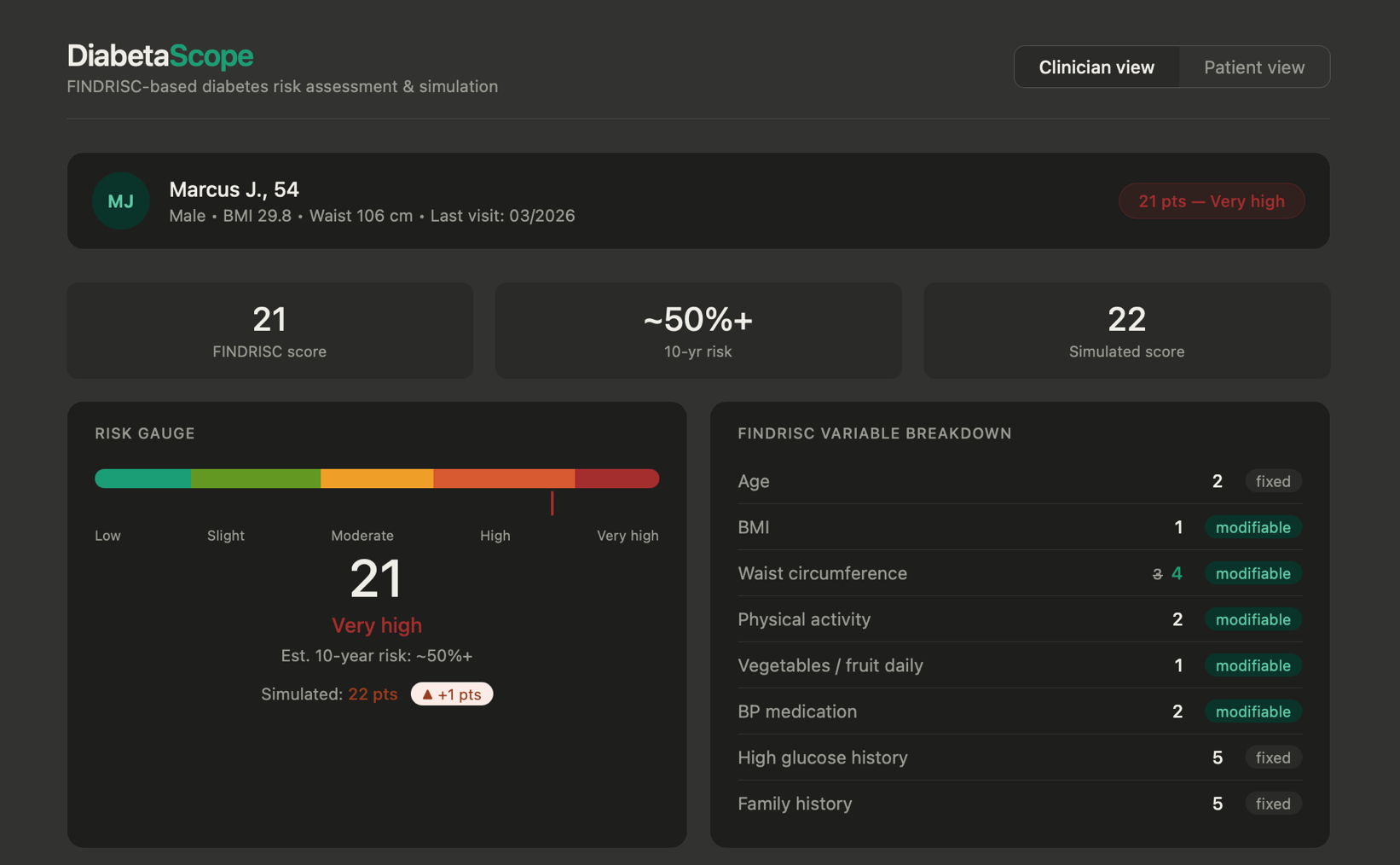
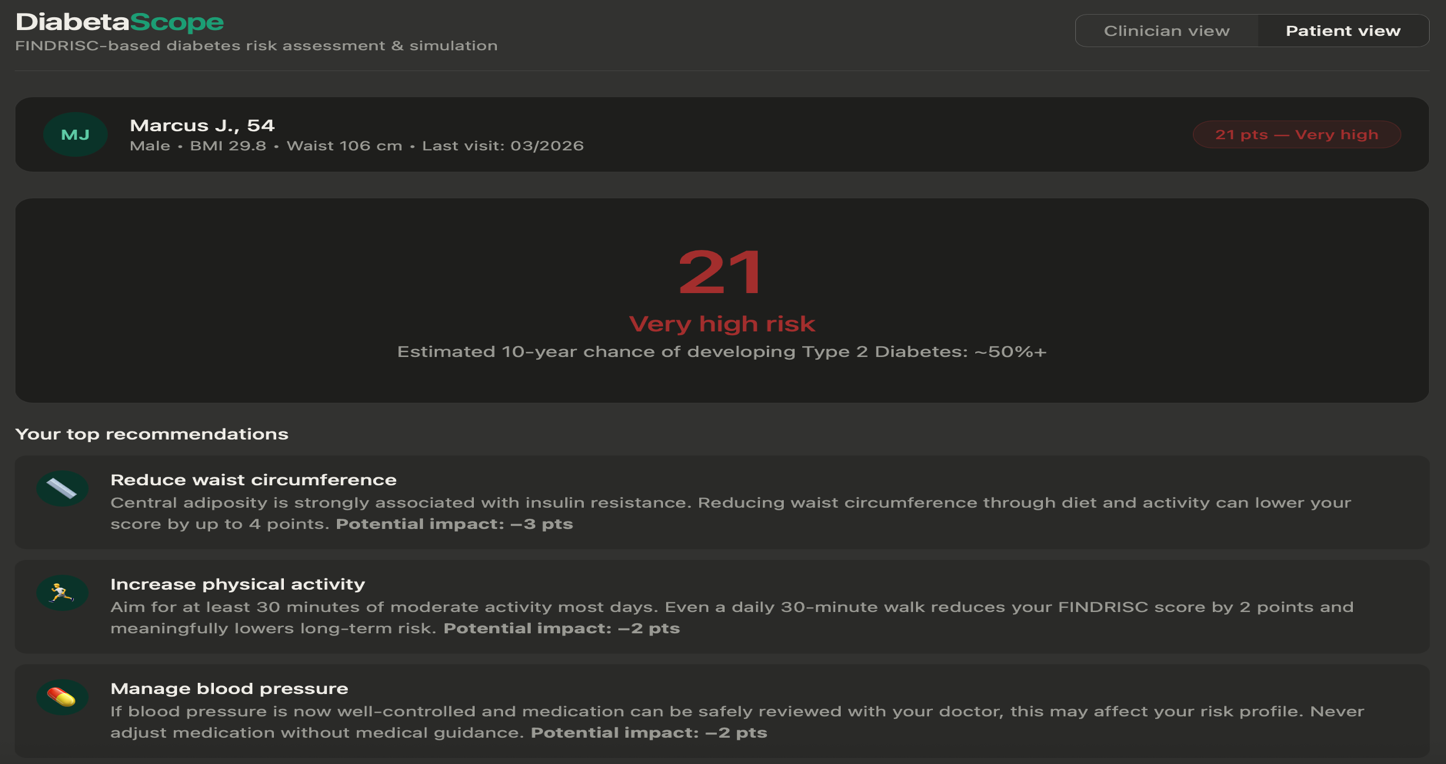
Over 500 million adults worldwide live with diabetes, and 4 in 10 don't know it. FINDRISC is one of the most validated screening tools for catching that risk early — but nearly every digital implementation of it does the same limited thing: takes eight inputs, spits out a score, and stops there. No simulation of what happens if something changes. No sense of which factor matters most for this patient. No version a patient can actually read. DiabetaScope was built to close that gap.
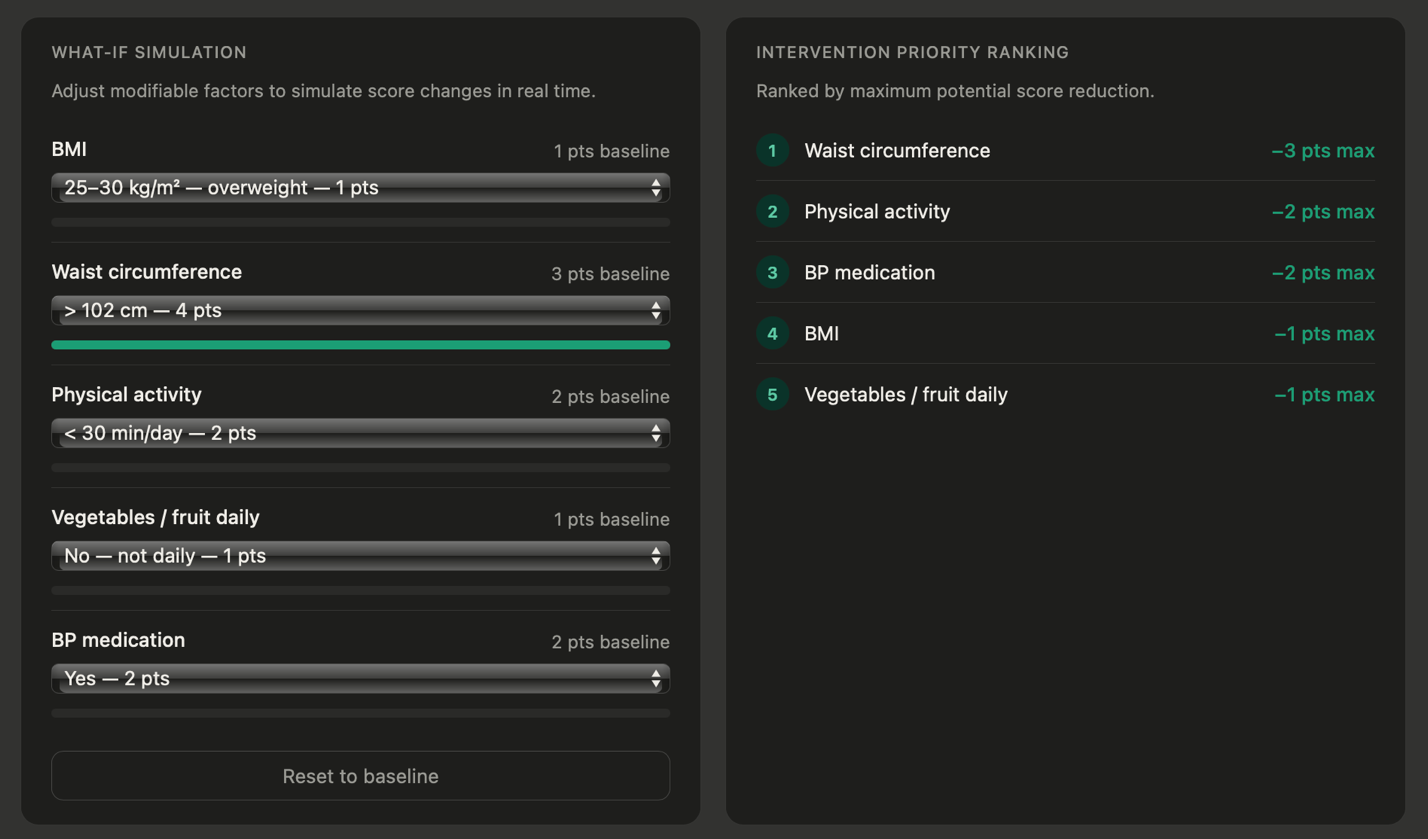
Improving all five modifiable variables for the synthetic patient — reducing waist circumference, increasing physical activity, eating more vegetables and fruit daily, and coming off blood pressure medication — dropped the FINDRISC score from 21 to 15, moving the patient from Very High risk toward the boundary of High risk. The trajectory chart makes the stakes visible over time: baseline risk climbing toward ~50% at year 10 versus a simulated ~33%, with the gap between the two lines widening every year.

DiabetaScope runs entirely client-side — no server, no database, patient data never leaves the browser. That wasn't a shortcut; it's a deliberate demonstration of a SMART on FHIR–style design pattern: the synthetic patient is structured as a JavaScript object that mirrors a FHIR Observation resource, so in a production deployment, that static object could be replaced by a live FHIR API call with no change to the scoring or rendering logic underneath. The architecture is the pitch as much as the prototype is.
The report is equally direct about the tool's limits: a single synthetic patient can't demonstrate population-level generalizability, FINDRISC's European derivation means U.S. deployment would need threshold recalibration, and any tool that presents a numerical risk score carries real risk of automation bias if a clinician treats it as more certain than it is. DiabetaScope addresses that last point directly in its interface — the score is labeled as an estimate throughout, not a diagnosis.
The live prototype is fully interactive — toggle between clinician and patient views, adjust any modifiable variable, and watch the risk trajectory update in real time.
Try the Live Demo →