A full deployment strategy for a 5-site, 37-provider women's health practice — built as IT Project Manager, from workflow redesign through technical architecture, interoperability, budget, and risk.
Virginia Women's Center — central Virginia's largest women's healthcare private practice, with 25 physicians, 12 mid-level providers, and 223 staff across 5 clinical sites — needed to move off an aging EHR that couldn't support interoperability, mobile access, or value-based care. I took on the role of IT Project Manager and built the complete deployment strategy: stakeholder governance, a redesigned clinical workflow, technical infrastructure, an interoperability framework, a phased 14-month rollout plan, a full risk register, and a revenue cycle management strategy — then presented it to a simulated executive leadership team.
Why It Mattered
The old system was actively limiting care.
$300K
annual transcription cost the new system was designed to eliminate
0
interoperability with hospitals, labs, or specialists under the old system
15+
MIPS quality points at stake in Promoting Interoperability compliance
14 mo.
target timeline to bring all 5 sites live
Clinical Workflow Redesign
Starting with one process, end to end.
Rather than redesign every workflow at once, I used the patient referral process as a worked example — mapping all 12 steps from a provider identifying the need for a referral through consult note return and closure, and tagging each step with the people involved and the specific EHR capability required to support it (electronic order entry, insurance eligibility verification, referral status tracking, interoperable direct messaging). The goal wasn't just to automate the existing process — it was to remove the points where referrals silently got lost.
Benefit realized in the redesign: structured readiness checks and status tracking throughout the referral lifecycle — reducing lost referrals, shortening time to specialty care, and giving the practice visibility into outcomes it never had with a paper-based process.
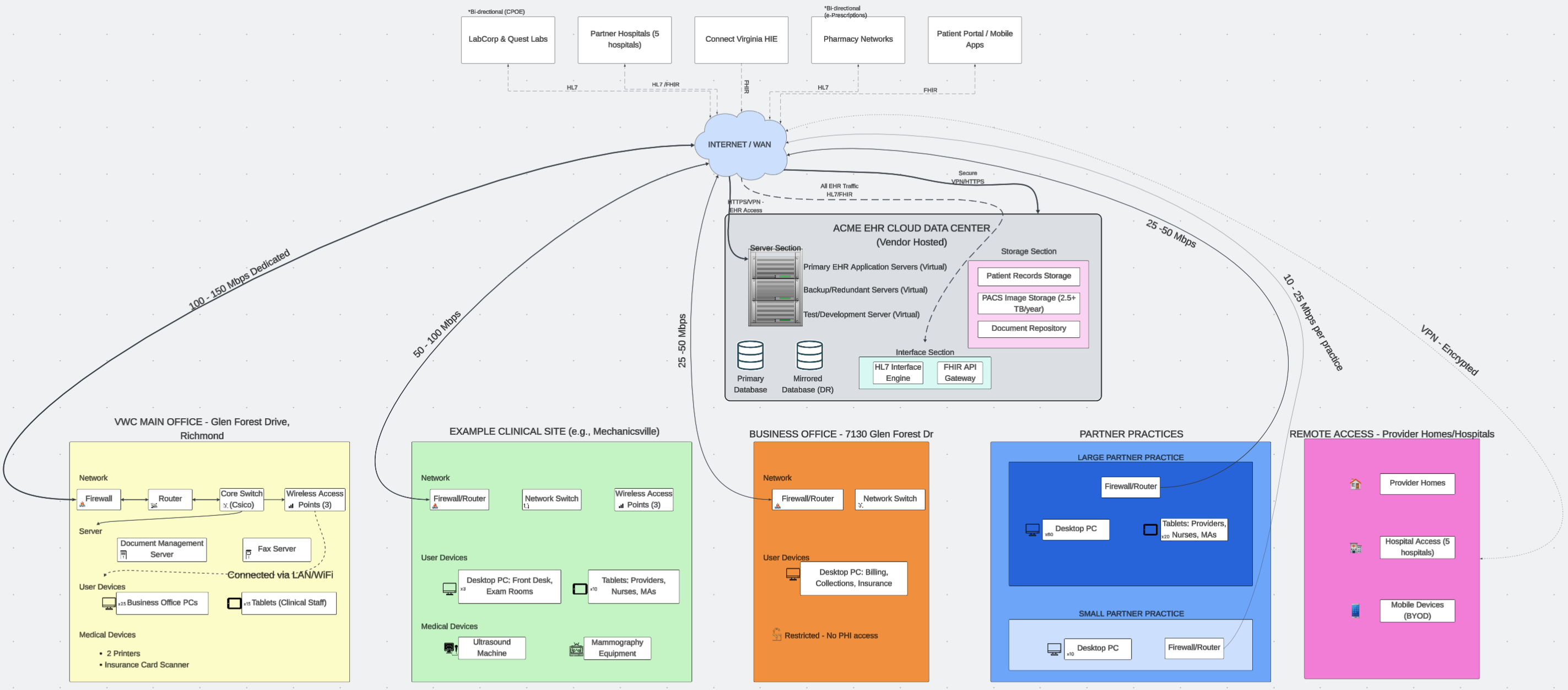
Technical Architecture
A hybrid cloud, hub-and-spoke design.
The architecture splits responsibility deliberately: a vendor-managed SaaS layer handles the EHR application, mirrored databases, and disaster recovery, while VWC retains local control over network, endpoint devices, and medical device integration — balancing cost, control, and HIPAA compliance across all 5 sites.
Rather than a single integration standard, I built a layered framework where each standard serves the use case it's actually strong at: HL7 v2.x for high-volume, transactional interfaces like lab results and hospital ADT feeds; CDA / C-CDA for structured care summaries at transitions of care, particularly hospital admissions; and FHIR APIs for everything modern — the patient portal, mobile provider access, the ConnectVirginia HIE, and future third-party tools. Underneath the transport layer, SNOMED CT, LOINC, and ICD-10 keep the clinical meaning of that data consistent across every system it touches.
Interface
Direction
Standard
Data
LabCorp & Quest
Inbound
HL7 v2
Lab results (auto-deposit)
Hospital L&D EHR
Bidirectional
CDA / HL7
Prenatal records, delivery summaries
PACS / Ultrasound
Bidirectional
HL7 / DICOM
Images, radiology reports
ConnectVirginia HIE
Bidirectional
FHIR
Patient data query & exchange
Patient Portal
Bidirectional
FHIR
Appointments, messages, results
Risk Management
Naming the failure modes before they happen.
Risk
Level
Mitigation
Physician resistance & low adoption
High
Phased rollout with reluctant adopters brought on last; dedicated physician champion; ongoing helpdesk
Productivity drop during go-live
High
Reduced schedules ramping 50%→67% over two months; overflow absorbed by other providers
Data migration errors
Medium
Preload only charts with upcoming appointments, within a 2-day window; old system available at first visit
Interoperability failures
Medium
Phased interface testing; 24×7 monitoring; message queueing to prevent data loss
Grounded in a Real Case Study
What actually happened when this played out.
This strategy was built against Virginia Women's Center's real, HIMSS Davies Award–winning EHR deployment — meaning the drivers, constraints, and outcomes referenced throughout aren't hypothetical. The real-world implementation this strategy is modeled on delivered a 19% post-implementation profit increase, an 11% rise in annual patient visits, and elimination of the $300K annual transcription cost — validating the phased, physician-championed approach this strategy is built around.
"The foremost factor that allowed VWC to enjoy EHR success was a culture of commitment and engagement at all levels." — VWC HIMSS Davies Award Application